09 Mar Face It® Partner News: For Years, KY’s most Vunerable Children were sent to other states for care be a state initiative is focused on bringing them home
She arrived at the Maryhurst home for girls in a police cruiser at only 12 years old.
She fought the staff; she refused to talk; she grunted and flailed and sniffed people.
Her uncle had molested her for years, beginning when she was 4, said Lou Smith, Maryhurst’s program manager, who has grown close to the girl. She was beaten and neglected, and by the time she got to Maryhurst in October 2012 her posttraumatic stress disorder was so profound that she slept only on her floor, fully dressed, and woke up screaming from the nightmares.
Until recently, the girl — whose name is being withheld to protect her identity — likely would have been sent to a psychiatric facility outside Kentucky at a cost to the state of possibly up to $500 a day. It’s a practice Kentucky followed for decades, shipping its most troubled, difficult-to-place children to hospitals out of state, some hundreds of miles from their communities and any family they had left.
But now the girl is instead headed to a foster home in Kentucky that is just miles from her older brother, the only relative she still trusts, said Judy Lambeth, Maryhurst’s president.
The Cabinet for Health and Family Services promised several years ago to fix the  fractured system that sent hundreds of the most vulnerable children in state custody across state lines, said Teresa James, commissioner of the cabinet’s Department of Community Based Services. The number of children in outof- state placements has since plummeted by more than 97 percent.
fractured system that sent hundreds of the most vulnerable children in state custody across state lines, said Teresa James, commissioner of the cabinet’s Department of Community Based Services. The number of children in outof- state placements has since plummeted by more than 97 percent.
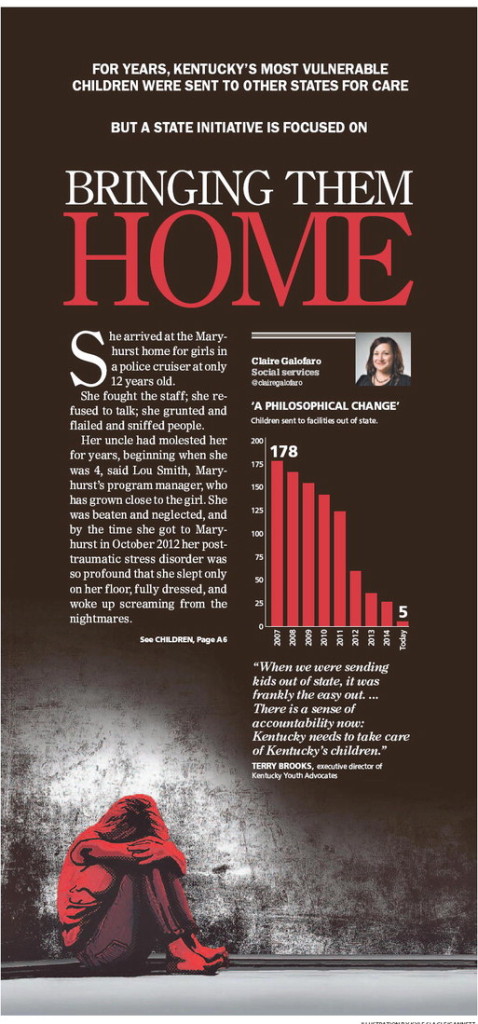
In 2007, 178 kids were in facilities out of state. Today, there are just five, according to the cabinet. It is a bright spot for a child welfare system bedeviled by the highest ever number of kids in state custody, now more than 7,700, and case workers so overwhelmed the cabinet struggles to keep its staff.
“When we were sending kids out of state, it was frankly the easy out,” said Terry Brooks, executive director of Kentucky Youth Advocates. “There has been a philosophical change. There is a sense of accountability now: Kentucky needs to take care of Kentucky’s children.”
‘It was a dream’
A decade ago, Kentucky did not have a coordinated network of providers equipped to handle children with a combination of the most severe behavioral problems, developmental disabilities or medical needs.
Georgia Swank, chief nursing officer for The Ridge Behavioral Health System in Lexington, calls them “the fall-between- the-cracks population” — the most helpless Kentucky citizens who had no place to go.
The children cycled in and out of hospitals and foster homes, often through dozens of placements, until the cabinet could find nowhere else in Kentucky able or willing to take them.
The providers were paid a bundled rate, an inflexible allowance for all wards of the state designated to require the highest level of care. It often did not cover the expenses necessary to safely treat the toughest kids: Many need oneon- one care every moment they’re not sleeping, or therapy that would require facilities to hire specialized staff.
Dozens of kids, at one point nearing 200, were turned away by every Kentucky agency. Then they were sent to out-of-state facilities that specialize in children with behavioral and cognitive problems.
James said the cabinet resolved to get every one of those children back to Kentucky before the end of Gov. Steve Beshear’s administration and send no more across state lines.
“It was a dream, I don’t think any of us ever believed we’d get here,” she said.
It required the state to rethink the way it handles the most difficult kids. State officials had to bring each child home individually, not using the onesize- fits-all approach to treatment and payment that created the problem in the first place, James said.
The state partnered with agencies like The Ridge in Lexington, Maryhurst and Uspiritus in Louisville, and Key Assets, a central Kentucky-based independent foster care agency.
One boy, living in a Texas neurological hospital at a cost to the state of $435 a day, was brought home to a therapeutic foster home in Kentucky. He now costs the state $189 a day and lives in a home with a family, James said.
“It’s one of those rare policy decisions that’s good for kids and good for the state budget,” Brooks said.
The number of kids in out-of-state placements dropped gradually each year for a few years, from 178 in 2007 to 123 in 2011, according to records obtained from the cabinet.
But in late 2011, Medicaid managed care companies began operating in Kentucky and forced the state’s hand. The companies started to refuse long-term hospitalizations for children outside the state, finding the pricy treatment — for some nearly $200,000 a year — was not medically necessary.
“It forced the state of Kentucky to step back, build a services system for all children, to ask, ‘How do we service them within our own state,’ ” James said.
The state created a system called “single-case agreements” that allows the cabinet, the agency that takes the child in and the Medicaid provider to create an individualized treatment plan. The state still pays the bundled per-day rate, but the managed care companies often agree to pay for additional treatment to avoid $500-a-day hospital stays.
The number of children placed out of state plunged from 123 in 2011 to 59 in 2012 to five as of last week.
Those five children are exceedingly tough cases, said Christa Bell, assistant director of the Department’s Division of Protection and Permanency.
One of them, a 15-year-old Kentucky boy in an Ohio facility was normal functioning until he was 7 years old, when he contracted a neurological illness. Now he cannot speak, he is not toilet-trained and sometimes acts out violently. He requires a caregiver at every moment of the day, sometimes two, and will for the rest of his life.
But the state has found that most kids returned from out-of-state hospitals have transitioned well into their Kentucky homes.
For instance, Bruce and Cindy Mchone, who live in Lexington and foster through the Key Assets agency, decided to foster a special-needs child when their own children grew up.
They took in a 9-year-old boy, their second full-time foster child, 10 months ago. He has autism and a long list of other special needs and the Mchones were warned he’d acted out violently. The boy had been in a secure hospital so long and grew so used to the environment he did not know how to open doors on his own. He was so terrified of traffic and noise he’d panic if they walked along a downtown sidewalk.
“A lot of people think these children need to be fixed, that they’re broken,” Bruce Mchone said. “They’re not broken. They just need a new way of reacting.”
The boy came into their home “like a tornado,” the Mchones said. He would awaken around 4 a.m. and talked constantly. He became hysterical if left alone, even for a minute, and they realized he’d been cycled through so many hospitals and homes he was scared they’d send him back again.
Cindy Mchone quit her job to care for him full time. Over the months, he’s calmed down, they said. He started calling them mom and dad. They took him recently to see “The Boxtrolls,” the first movie he had ever seen in a theater.
“You don’t see the child when you first bring them home,” Cindy Mchone said. “All you see is their pain and suffering, their anger. But if you keep working with them, eventually that child comes out. I just hope that when he looks back at when he was little, he can think about a positive time, rather than always having to remember all the things he had to go through that got him here.”
Their job is to prepare him to move into a permanent, adoptive home, whenever he’s ready.
‘She just needed hope’
Most believed that little could be done for the 12-year-old girl who arrived at Maryhurst in a police cruiser, that she would spend most of her life confined in a hospital.
Smith recalled that she looked “primitive,” her hair was matted, like it hadn’t been washed in a year. She couldn’t speak, she made only grunting noises and usually refused to use a toilet.
Months later, once the child started talking, Smith learned that she could recall every second of her abuse. It played over and over in her mind, on an endless, inescapable loop.
Maryhurst hired part-time staff so a therapist could be with her, only her, for 12 hours every day. She required behavioral therapy, speech therapy, occupational therapy, medication, a specialized classroom — a combination of treatments impossible under Kentucky’s old model of child welfare, Lambeth said.
They discovered soon that the child has an exceptional mind. She read a book about the cerebral cortex, quizzed her therapists on their moods and taught them why their brain made them feel that way. She makes eye contact now, she talks, and laughs.
“She just needed hope,” Smith said, “something to look forward to, somebody to care about her.”
Reporter Claire Galofaro can be reached at (502) 582-7086. Follow her on Twitter at@clairegalofaro.
Read more here: http://www.courier-journal.